

Death by neck hug
More than you wanted to read about choking


Note: The following contains discussion of both consensual and non-consensual choking, strangulation, domestic violence, and a variety of adverse events including stroke, death, and moral panic. I (Chesed) agree with the research consensus that most sexual “choking” would be more accurately called “strangulation.” However, I will mostly default to calling consensual, sexual neck grabbing activity “choking” to match common usage. Nothing in this article is medical or legal advice, although you may feel free to imagine me as a sexy nurse.
Choking discourse is back. Or rather, was back. I’m sure by the time I publish this, Twitter will have moved onto the next hot topic. Do bald men have souls? Do sluts have easier births? Is handwashing a scam cooked up by Big Soap?
As far as I can tell, the conversation was kicked off by a Guardian article by Anna Moore, highlighting a new study examining the relationship between sexual strangulation and markers of brain damage. The study is interesting. The article is inflammatory, one-sided, and misleading.
I agree that choking is worth discussion. It’s common and potentially dangerous, and may be growing in popularity. As a lady who likes to be choked, I am very interested in the true risk of sexual choking and the mechanism of potential harm. Before diving into the evidence, my practice was to engage in very limited choking. After reading as many papers about the physiology and potential harms of choking as I could, my practice will remain the same. Some of what I read was illuminating. This article was not.
Almost every claim in the article is misleading, based on research which doesn’t cleanly apply to consensual sexual choking or offers limited insight:
Sexual choking “can also lead to difficulty swallowing, incontinence, seizures, memory problems, depression, anxiety and miscarriage” — misleading, based on victims of non-consensual strangulation during sexual/domestic violence
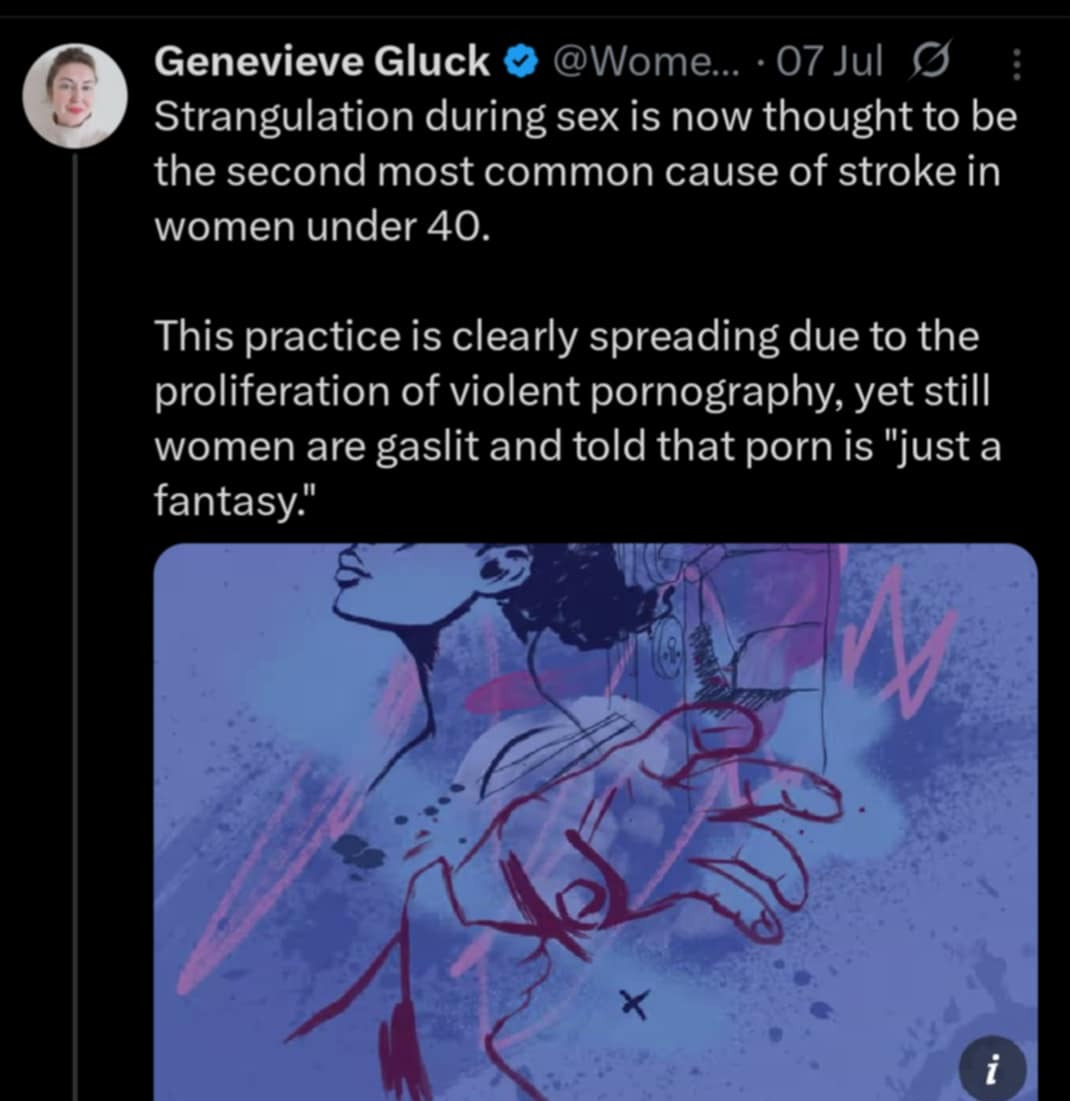
Sexual choking is “thought to be the second most common cause of stroke in women under 40 — misleading and likely untrue, based on bad math and victims of non-consensual strangulation during sexual/domestic violence
Choking has become very prevalent among young people — accurate
Choking is more dangerous than waterboarding — probably true, but irrelevant
Women who have experienced frequent sexual strangling (>4 times in the last month) show higher levels of S100B, a marker of brain damage — accurate description of a study, unclear if this means anything
Women are pressured or forced into choking during sex/choking is for male pleasure — not supported by research
The increased prevalence of choking during sex is due to porn — have yet to research, seems plausible
There is a growing number of women and girls killed or injured in violence that their male perpetrators claim was consensual — have yet to research, seems not actually very common (but bad)
I will address claims 1-6 in this post. In future posts, I hope to address 7 and 8, and go more into depth on the known risks of choking.
Claim 1: Sexual choking leads to “…difficulty swallowing, incontinence, seizures, memory problems, depression, anxiety and miscarriage”
The source for this is a paper published in Neuropsychological Rehabilitation, “The neuropsychological outcomes of non-fatal strangulation in domestic and sexual violence: A systematic review”, written by Helen Bichard, Christopher Byrne, Christopher Saville, and Rudi Coetzer. The paper is a systematic review of 30 peer-reviewed studies looking at the impact of non-fatal strangulation in the context of domestic and sexual violence. In other words, none of the studies looked at consensual choking.
What if we tried to understand the impact of vaginal sex by examining women who presented to hospitals or police stations after surviving sexual assault or domestic violence? It is incredibly misleading to present the risks of being choked by someone who actively wants to hurt you (e.g., rapist or abusive partner) to the risks of being choked by someone who is actively trying to avoid hurting you (e.g., your boyfriend or sex buddy). I already know that it is possible for men to kill or permanently harm me through choking/strangulation. The question is whether a man can safely use a small fraction of his strength to choke me without harming me.
I’m sure that everyone who comments “biased sample!” under Aella’s sex research tweets will join me in condemning the Guardian’s reporting.
Claim 2: Sexual choking is “thought to be the second most common cause of stroke in women under 40.”
Some researchers looked at causes of stroke in young people and found that head/neck trauma is a relatively unusual risk factor. Top risk factors include high cholesterol, smoking, high blood pressure, family history, high BMI, migraine, and oral contraceptive use (Ekker et al., 2022).
So where did this alarming statement comes from? The Guardian links to Bichard et al. (2022) again, who in turn cite…well, it’s unclear:
Another unpublished thesis demonstrated a 10-15 fold increased risk of stroke amongst women under 40 who had suffered IPV (n = 237) versus a matched control (Smith, 2009). Smith demonstrated significant associations between strangulation, loss of memory, paralysis, and stroke. Combining this with the incidence figures for strangulation gives substance to the warnings elsewhere in the literature that strangulation may be the second most common cause of stroke in women under 42, and should be included in the differential diagnosis of younger patients, particularly in the context of apparently spontaneous arterial dissection (Clarot et al., 2004; Malek et al., 2000; Milligan & Anderson, 1980).
Let’s begin with Smith (2009), the unpublished thesis. Smith surveyed 237 women (18-56) exposed to interpersonal violence, 5 of whom reported having experienced a stroke (3 ischemic, 2 hemorrhagic). She uses an Oxford database to estimate the expected incidence of stroke for women in the UK aged 20-44 (0.14/1000/year). Smith then compares a subset of the women (209, limited to align ages with the control) to the control (expected incidence based on age and gender) and finds that women exposed to interpersonal violence had an 10-15x higher incidence of stroke than would be expected based on their age and gender.
What does this tell us? Well, if you are a victim of interpersonal violence in the UK, this study suggests you are more likely to have experienced a stroke than if you are not a victim of interpersonal violence in the UK. Remember, the “control group” was matched on only age and gender. Any and every other risk factor for stroke (smoking, blood pressure, other medical conditions, diet, poverty, drug use, health, genetic factors, medication) might vary between the sample (women affected by interpersonal violence) and the rest of the population. For example, Smith notes that women exposed to interpersonal violence are more likely to smoke (62% sample, 22% population) and drink >3 units of alcohol a day (31% sample, 24% population).
This does not tell us that sexual choking is the second leading cause of stroke for young women. It doesn’t even tell us that exposure to interpersonal violence increases the risk of stroke, although I wouldn’t be shocked if it did. Is there a smoking gun I’m missing in the other cited studies? No. Each is a case study of women suffering carotid artery dissection or occlusion (and often stroke) following non-consensual strangulation in the context of domestic violence (Clarot et al., 2004, Malek et al., 2000, Milligan & Anderson, 1980). Based on these studies, one could reasonably conclude that when a young woman has a stroke, clinicians should consider violence as a possible underlying cause. However, there is nothing to support the claim that sexual choking is the second most common cause of stroke in women under 40.
Claim 3: Choking has become very prevalent among young people
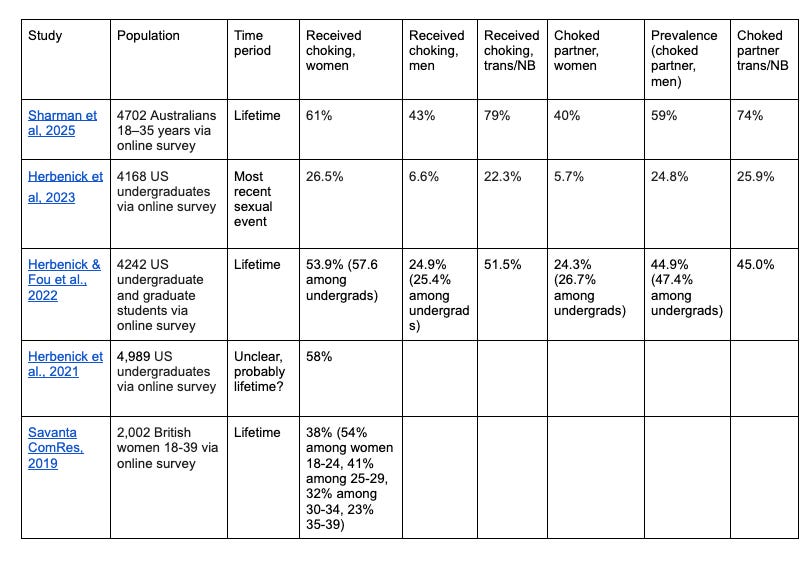
There’s at least one thing that Moore and I agree on — sexual choking is common. Studies at US universities suggest ~25% of young women received choking in their last sexual encounter, and 50-60% have been sexually choked at least once (please see the table below for study details). The prevalence seems to be similar in the UK and Australia. In every study I’ve reviewed, choking is more common among younger women. This is true for lifetime experience, not just recent encounters, suggesting that choking may be becoming more popular over time.
Claim 4: Choking is more dangerous than waterboarding
This claim, of course, cites Bichard et al. (2022) again:
In waterboarding, however, it is only the airway which is occluded. Strangulation is potentially more lethal: not only is breathing interrupted, but also blood flow to and from the brain. As such, it can carry all the consequences of other hypoxic-ischaemic injuries such as cardiac arrest, but with the additional trauma reactions evidenced in the studies we reviewed.
I agree, by the way, that strangulation is probably more lethal than waterboarding. I don’t think you have much of a window between strangling someone hard enough to scare a hardened prisoner and strangling someone hard enough to make them pass out or die. The whole point of torture is to be very unpleasant without actually killing someone. This doesn’t really have much to do with anything. The reference seems like another attempt by the Guardian to show that Experts Say that choking is bad while repeatedly citing the same paper (which again, is about choking in the context of sexual and domestic violence).
Claim 5: Women who have experienced frequent sexual strangling (>4 times in the last month) show higher levels of S100B, a marker of brain damage
I actually thought that the Guardian reported on this study very reasonably, simply noting the methodology and key findings:
In a paper published in May, 32 young women were recruited from a large midwestern university in the US and separated into two groups – those who’d been strangled at least four times during sex in the last 30 days and those with no history of strangulation. (There were 15 from the former group and 17 in the second.) Blood was taken from all recruits. The samples from the women who’d been strangled showed elevated levels of S100B, a marker of brain damage.
Huibregtse et al. (2025) found no significant difference between the choked and unchoked groups in 4 out of 5 biomarkers studied. However, one biomarker, S100B, was significantly higher in the group with recent, frequent sexual strangulation.
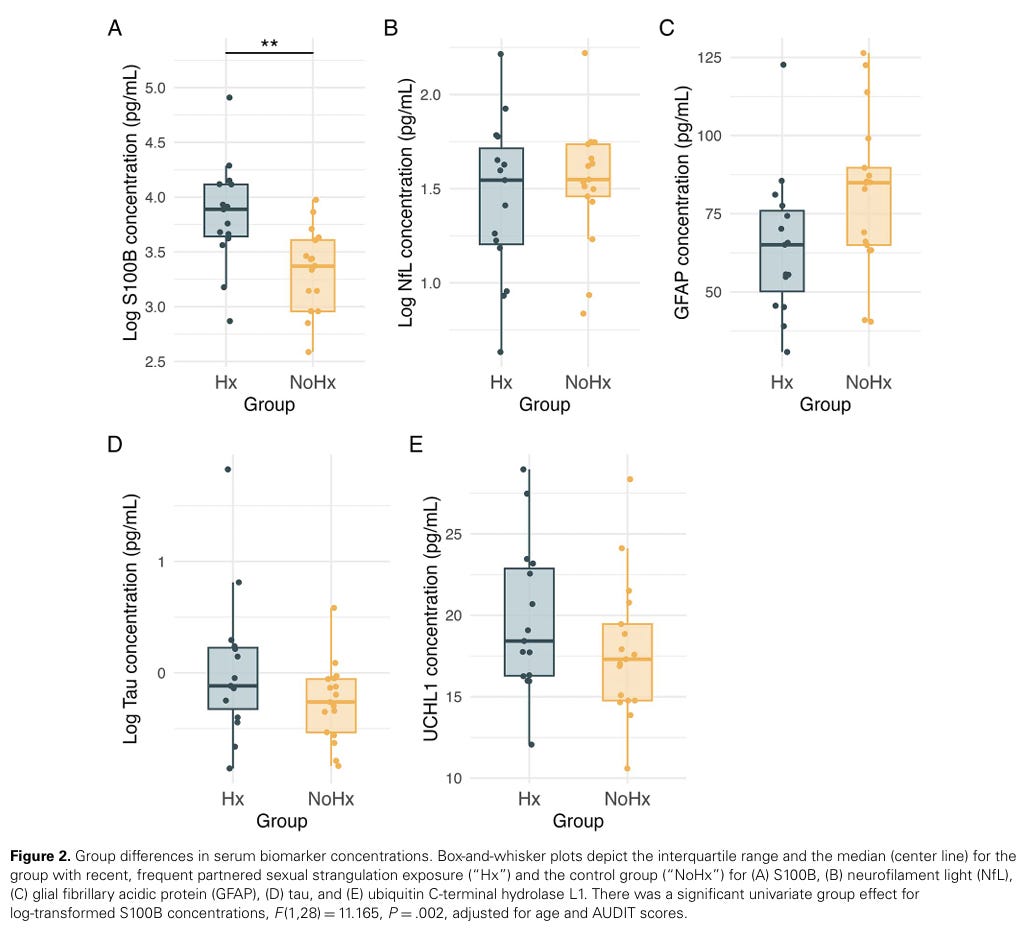
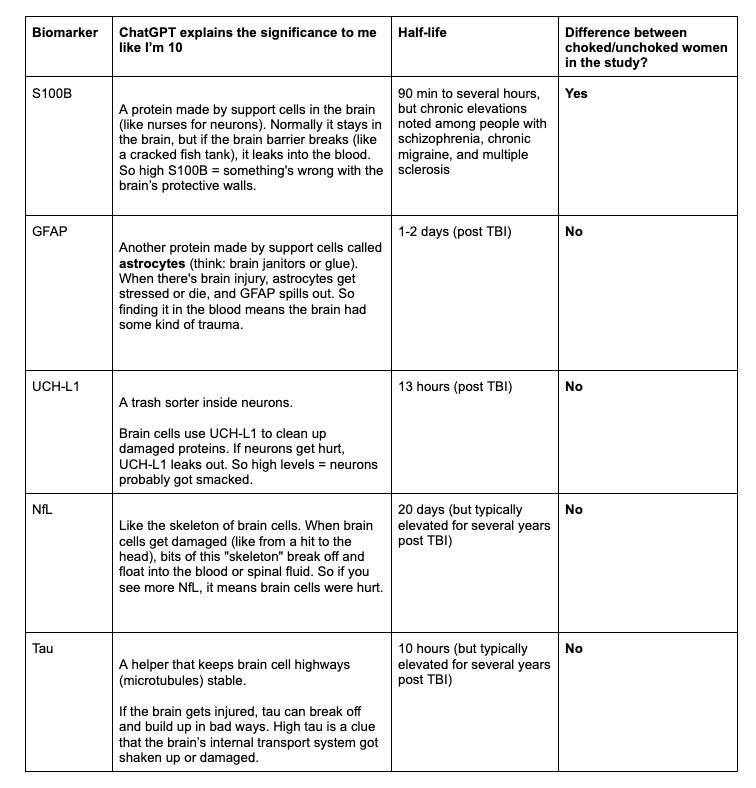
The biomarkers include: astrocytes: S100B and glial fibrillary acidic protein [GFAP]; axons: neurofilament light [NfL] and glial fibrillary acidic protein [GFAP]; neuronal body: ubiquitin C-terminal hydrolase L1 [UCHL1]. The authors note that “UCH-L1 and GFAP are approved by the US Food and Drug Administration as a dual biomarker blood test to rule out the need for a computed tomography (CT) scan following mild TBI.”
A few thoughts:
We should be cautious in making grand conclusions from a n=32 study. With a small sample size, it’s more likely that a statistically significant result will not generalize to a larger sample size or could overestimate the real impact.
We don’t know if frequent choking causes elevated S100B or if the two are simply associated. It could be the case that women who like to be choked a lot are different from women who don’t get choked at all in ways other than just the choking. Is it possible that women who like choking more are more physically or emotionally stressed? Exercise and physical/emotional stress are also linked to elevated S100B. So are certain mental health issues (e.g., bipolar, depression).
The authors hypothesized that all of the biomarkers would be elevated in women with frequent exposure to sexual choking. Is there an explanation for how choking causes brain damage in which it makes sense for S100B to be elevated without any of the other markers of brain injury being elevated? Is S100B especially sensitive?
If frequent sexual choking does lead to S100B elevation, is that elevation dangerous? Is it clinically significant? It would be interesting to see a similar study that used clinically significant measures like headaches and other neurological symptoms or short/long term memory.
Claim 6: Women are pressured or forced into choking during sex/choking is for male pleasure
Moore’s Guardian article implies that women are choked during sex due to pernicious external forces: social pressure to not be “vanilla”, a desire for male validation, and the normalization of choking in online porn. Neither Moore nor the sex researchers she cites spend much time discussing the role of pleasure.
In Frequency, Method, Intensity, and Health Sequelae of Sexual Choking Among U.S. Undergraduate and Graduate Students”, Herbenick and friends surveyed over 4,000 US college students and asked about choking in detail (Herbenick & Fou et al., 2022). Among students who had received choking during sex, 92.1% of choking instances were consensual. Most respondents who had been choked had only ever experienced consensual choking: 76.5% of women (n = 864), 85.6% of men (n = 286), 63.6% (n = 28) of TGNB+ (trans and non-binary) participants.
While any amount of non-consensual choking is horrible, the answer to “Why are women getting choked?” is not “It’s rape, stupid.” But what is it? Herbenick & Fou et al., 2022 aren’t sure — “Yet, for a sexual practice that is consequential to health and potentially lethal, we were struck that a minority of participants (albeit, a sizable minority) described being choked as “very pleasurable.” If it is not very pleasurable and yet carries significant risks, it is curious how choking has grown so quickly in prevalence.”
When the authors note that a “sizable minority” of participants described choking as “very pleasurable” they mean 41.1% of all participants. Another 33.8% described choking as “somewhat pleasurable.” Among both undergraduates and graduate students, more women rated choking as “very pleasurable” than men. Just 5.9% of participants reported that they didn’t like choking but “I’ve let partner(s) do it because they seem to like it”. Submitting to choking to please a partner was actually more common among men than women, although I’m not certain that the difference was significant. Additionally, ~85.3% of women respondents reported feeling pleasurable sensations/euphoria from choking (81.7% among all of participants, 73.3% men, 82.7% TGNB+).
The data the authors have collected doesn't really match the narrative they (and the Guardian) seem to fixate on. Influence from the media, porn, poor sexual communication norms, and weird gender stuff may have contributed to choking going mainstream and associated negative effects. But a discussion of why people engage in sexual choking should acknowledge that a lot of people (including women!) enjoy the experience of being choked.
I reviewed a qualitative study incorporating interviews from 24 young women 18-33 with experience receiving (all 24) and giving (13/24) choking during sex (Herbenick & Guerra-Reyes et al., 2021).
Combining their interviews with my personal experiences, I found a few common themes that choking can evoke for women:
Intimacy, safety, and affection (this man will take care of me, I trust him, etc.)
Submission/possessiveness/lack of control (I can’t move, I have to listen to what he says, he’s in control, etc.)
Pleasurable fear (He could literally kill me, omg he’s so strong !!!!!, I wonder what he’s going to do to me, ooh he has a scary/wild look in his eyes, etc.)
Arousal (obviously)
Physical sensations (head rush, heightened orgasm)
What’s going on with non-consensual choking during theoretically consensual sex?
Herbenick, Patterson, et al., (2021) found that most students were never (21%) or sometimes (32%) asked for consent before receiving sexual choking. This doesn’t mean the students perceived the choking as negative or non-consensual, which seems to be a less common experience. This matches my own experience in college hookups — some men choked me, nobody asked. Luckily for them, I liked being choked! However, being choked without negotiation can be unpleasant or even terrifying.
If you trust your partner, or trust the social environment you’re in, you might lightly push at his hands or screw up your face and say “No, thank you!” Unfortunately, if someone is choking you they can kill you very quickly. They probably don’t have any intention of doing so, but it’s pretty hard to make that judgement call when a man’s hands are around your throat. Without prior discussion, there’s no way to know if his response to a “No” would be a rapid apology or tightening his grip. Especially if you are in an isolated place or afraid to call for help, it may feel like the best response to unexpected choking is to play along and hope you aren’t murdered. This is really awful and terrifying, and I don’t want to downplay the negative impact of nonconsensual choking.
Conclusion
I remain frustrated that the Guardian chose to publish an unbalanced, poorly researched, and often misleading article. To credibly communicate risks (and risk mitigation), I think it is critical to avoid lying or making overconfident conclusions from limited evidence. The experts cited in the Guardian article repeatedly scoff at the notion of risk mitigation or safer choking, seeming to propose a choking abstinence only approach. I do not think this is likely to be effective. In fact, I think it might be counter-productive.
The public health community received a lot of pushback during the COVID-19 pandemic for making sweeping, paternalistic recommendations based on the idea that people cannot understand risk or make their own risk/benefit decisions. With choking, they seem poised to repeat the mistake. If roughly half of college women have been choked during sex, do you think they are likely to listen to authorities that breathlessly link it to stroke, seizures, and incontinence? Or might they conclude that the authorities, as usual, are full of shit?
I suspect that sorority presidents are not reading SlutStack. But for what it’s worth, my own safer choking practices are as follows:
Do not let strange men choke me. In fact, I avoid being alone with men I don’t know and trust. In the sexual community I am part of, sexual choking is not allowed by default, and requires negotiation and awareness of safer practices. Any man who choked me without negotiation would be risking his reputation.
Use a safe gesture (triple-tapping).
In negotiation about choking:
Encourage men to fake choke or threaten to choke (e.g., put hands on sides of neck without pressure, put pressure near collarbone).
Ensure men know to avoid the trachea and the front of the neck in general.
Ensure men know that I do not want to pass out/get dizzy.
Enjoy safer alternatives to choking that create a similar headspace.
Next steps
Future posts will address:
What is choking anyway?
What else do we know about the risks of sexual choking?
Why do people enjoy sexual choking? Is it because of porn?
How do young men and women perceive choking? What safety measures, if any, are they taking?
How common is the “rough sex” defense (i.e., men getting away with murder by strangulation by claiming it was consensual)?
What about breath play?
Balanced article, thanks for writing it. I was taught how to choke ‘correctly’ by a man with more BDSM experience than I but I do think it’d be a public service to have an article (with drawings ; or a video) about how to do it safely.
Re. Men enjoying choking their partners - I’m still too concerned about executing the choke correctly to really find the extra dominance/the extra fake threat truly arousing. IMHE, fake fighting/fake wrestling does that better. I imagine that’s why less men than you’d expect actually enjoy it. We do it for our partner(s)’ pleasure.
Re. non consensual choking. Look, I get that fawn is an instinctive response but it’s going to be really rare that saying or indicating “no” is going to lead to your murder. Think about it from the man’s pov. Even if you were unlucky enough to have sex with the kind of man who would ignore his partner’s wishes, what would he do with the body? I don’t know how to study that but, IMHO, you’re not making things worse by indicating your boundaries. The main thing you might lose is the illusion that that guy IS the kind of person who would respect your limits.
As a man, I'm not really into it but women I've been with have wanted to be choked and so I've done it for them. The study on how often people have been choked should have also asked how often people do the choking and who initiated it